


The physicians at VIRGINIA GASTROENTEROLOGY participate in GIQuIC, the GI Quality Improvement Consortium, a medical registry utilized by gastroenterologists in the United States. Physicians contribute procedure data to GIQuIC which is then analyzed so adjustments can be made to allow us to continuously improve the quality of care we provide to our patients. The data in GIQuIC is also used to advance research and develop guidelines for care across the field of gastroenterology.
GIQuIC is a powerful tool in the fight against colon cancer and we use it to look at a number of different measures to ensure our procedures are as thorough and effective as possible. Below are three measures we track against the national goals that have been set by the GI societies.
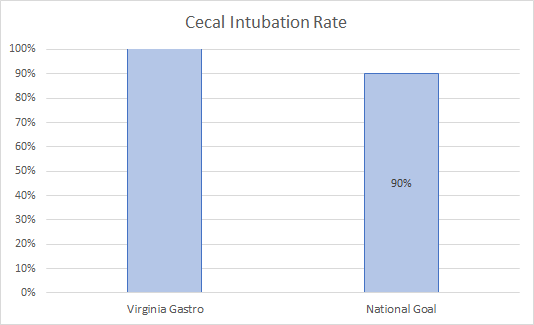
Cecal Intubation Rate
The goal of a colonoscopy is to advance the scope all of the way to the cecum and that is measured by Cecal Intubation Rate. The national standard for doing so has been set at 90% by the GI societies.
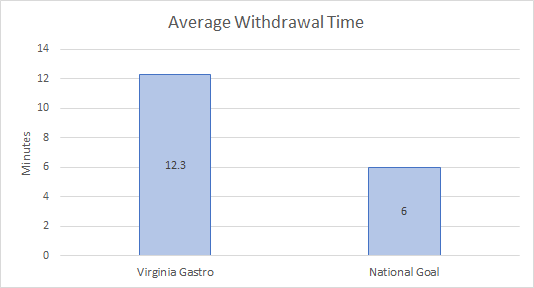
Average Withdrawal Time
Once the cecum is reached, the endoscopist will withdraw the scope while searching for adenomas. Adenomas are a type of polyp that can turn cancerous so it’s important to identify and remove them during a colonoscopy. It has been determined that the withdrawal time should be no less than six minutes to ensure a thorough examination.
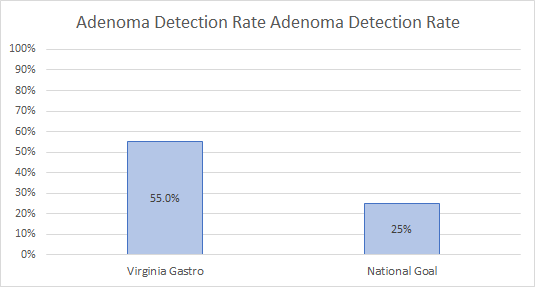
Adenoma Detection Rate
Adenoma Detection Rate, or ADR, is considered to be the most important quality indicator for a gastroenterologist and it calculates the percentage of time that at least one adenoma is detected during a colonoscopy. In fact, for every 1% increase in ADR, colo-rectal cancer rates decrease by 3% and morbidity decreases by 5%. The GI societies have set a national goal of 25% for Adenoma Detection Rate in screening colonoscopies.